Discuss the factors which influence the out come of surgical treatment for primary post partum heamorrhage and evaluate the different surgical techniques.
Factors
- Use of pharmacological agents should not delay the recourse for surgery
- Multidisciplinary team / team work and experienced staff
- Counseling the patient and family
- Availability of theater/ blood and blood component transfusion
- Availability of HDU/ ICU
- To identify the cause of heamorrhage ( Atonic, placenta previa, placenta acreta , rupture
- Future aspiration for reproduction
- Decision to do hysterectomy should be taken by the most senior staff
- Sequence of action (treatment) should be executed without delay ( Non invasive to invasive)
- Early recourse to hysterectomy associated with placenta previa, uterine rupture
- In emergency situation for atonic uterus, subtotal hysterectomy is the treatment of choice (Quick and less complication)
- Prophylactic antibiotics
Evaluations of the surgical technique
- Suturing of the vaginal and cervical tear +/- packing
- Can be done in the labour room
- Need good light
- Should be gentle as tissues are soft and friable
- Balloon tamponade
- Replace uterine packing
- First line surgical treatment for atonic uterus
- High success rate ( 80%)
- Less invasive
- No General anesthesia
- Can be done in the labour room( No time wasted)
- Simple – less cost with condom catheter
- Can be practice in low facility institution
- Immediate response
- Avoid hysterectomy
- Haemostatic sutures ( B Lynch, modified B lynch)
- Very successful ( Over 90 %)
- Reduce risk of hysterectomy
- All methods are equally effective
- Complications are rare ( Pyometron or uterine necrosis)
- Immediate results
- Invasive
- Need anesthesia
4. Selective arterial occlusion or embolization by interventional radiologist
- Non availability of facilities and expertise in most centers
- First line treatment for placenta acreta or previa where intra-arterial balloon are placed in radiology department before the woman goes to theater for caesarian section.
- Does not impair menstruation or fertility later
- Complications are rare but disastrous ( Occlusion of femoral arteries)
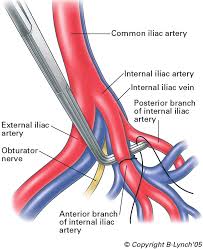
- Internal Iliac or Uterine artery ligation
- Invasive
- Efficacy is less (40%)
- Better results in uterine artery ligation
- Damage to the ureter and internal iliac vein
- Future fertility and pregnancy unaffected
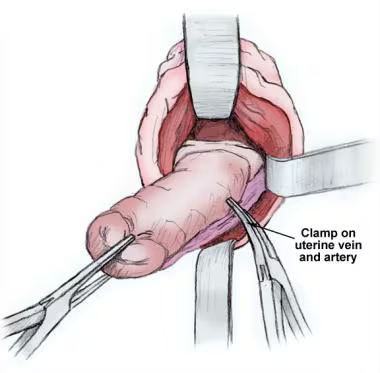
- Hysterectomy
- Subtotal hysterectomy is treatment of choice for atonic uterus
- Risk of developing neoplasia in the cervical stump – several years later should not be relevant in life threatening situation
- Cervix difficult to identify in a post partum fully dilated uterus there for total procedure may be complicated with bleeding leading to prolong surgery due to difficulty in identifying the vaginal angles
- Total hysterectomy is the treatment of choice in major degree placenta previa and placenta acreta
- Help of a experience surgeon
- In placenta acreta high chance of bladder and ureteric damage- prophylactic ureteric stenting and bladder catheter
7. Pelvic packing in extreme situation